Metastatic Castrate-Resistant Prostate Cancer

Dr. Catalona has written articles and answered questions on the topic of hormonal therapy in previous issues of QUEST, but new therapies are rapidly becoming available, and previous articles are no longer up-to-date.
This article provides information on and an explanation of the newest therapies available for advanced prostate cancer treatment, referred to as Metastatic Castrate-Resistant Prostate Cancer.
Initial treatment for prostate cancer hasn’t changed all that much in recent years. And after that initial treatment, if PSA is negligible, no other treatment is indicated.
If PSA begins to rise after initial radical prostatectomy, the next treatment is most often salvage radiation therapy. With a continued rise, the next line of treatment would be hormonal therapy.
In that situation, conventional hormonal therapies are prescribed: usually beginning with injections that dramatically decrease the production of male hormones from the testicles (e.g., Lupron, Zoladex, etc) and an initial course of pills (e.g., Casodex) that block the testosterone flare-up response that occurs with these injections.
Hormonal therapy is meant to target or block the production of male hormones, called androgens, that control the development and maintenance of male characteristics. Theoretically, it would stop the growth of prostate cancer cells that need androgen to reproduce.
Problem
But prostate cancer cells aren’t so easily stopped. We know that prostate cancer at some point becomes resistant to withdrawal of testicular androgens. Just as insects to insecticides and antibiotics to bacteria, the prostate cancer cells develop resistance to conventional hormonal therapy.
Sometimes, the cancer cells themselves produce their own androgens and continue to stimulate their own growth. In this case, pills and injections are not stopping the prostate cancer cells, and they start to multiply again.
That condition, which previously was called androgen–refractory prostate cancer, is now called castrate-resistant prostate cancer because, now, we know that even if androgen production is being shut down from normal body tissues (e.g., testicles, adrenal glands, fat, etc.), the hormonal therapy is not stopping prostate cancer cells from producing the androgen they need to grow and reproduce.
First-Line Treatment
The first-line chemotherapy for that stage of castrate- resistant prostate cancer is an every 3-week dose of docetaxel with prednisone, and as long as it’s working, nothing more is done.
Up until two years ago, no additional treatments were available for metastatic castrate resistant prostate cancer (mCRPC) so not much more could be done. The prognosis was not good and symptoms, including bone metastases, were very painful.
New Therapies
Now, new therapies are directed to this stage of metastatic castrateresistant prostate cancer, with one of the primary considerations being protection of the bones from fractures caused by bone metastases or fractures caused by osteoporosis resulting from hormonal therapy.
Chemotherapy is not usually recommended until there is definite evidence of metastases.
The therapies described below have recently received FDA approval.
These new therapies provide longer survival for those in treatment than those in the control group or taking a placebo.
But using these new treatments is challenging: side effects are numerous and careful monitoring is essential.
Jevtana (cabazitaxel)
When docetaxel no longer works, Jevtana (cabazitaxel) was recently FDA approved as second-line chemotherapy for the next treatment.
For a short while, Jevtana was the first and only therapy to provide significant survival benefits in secondline metastatic hormone-refractory prostate cancer.
It is still used as the preferred next treatment but other agents have since been FDA approved, and they are often prescribed next instead of docetaxel.
Abiraterone Acetate (Zytiga)
Zytiga is a pill, used along with prednisone, to target bone metastases from prostate cancer that no longer respond to chemotherapy.
The FDA approved Zytiga only for patients who previously had chemotherapy, and it is extremely expensive.
A recent study showed the treatment is beneficial both in patients who have and those who have not received chemotherapy, but, again, it is only currently approved for those who have received and failed chemotherapy.
Patients in the clinical trial who received a combination of Zytiga and the steroid prednisone were 57% less likely to see their cancer advance. The treatment also delayed the onset of pain and the need for further chemotherapy.
Enzalutamide (Xtandi and formerly called MDV3100)
Enzalutamide targets multiple steps in the androgen-receptor-signaling pathway, the major driver of prostate cancer growth.
It is one of the new drugs than can interfere with the action of androgens produced by the prostate cancer cells themselves.
It significantly prolonged the survival of men with metastatic castration-resistant prostate cancer after chemotherapy.
Sipuleucel (Provenge)
I include Provenge because it is FDA approved, but I question its use. It didn’t appear to affect disease progression and no evidence was presented to show it killed tumors. Evidence showed that it appeared to prolong life for a few months.
Still, for men with late-stage prostate cancer, it seemed to provide hope that a new type of therapy, in this case, immunotherapy, could prolong life by a few months and with more research provide real help.
I haven’t found any reasons to support the use of Provenge (See QUEST, Summer/Fall 2012, page 9 on www.drcatalona.com)
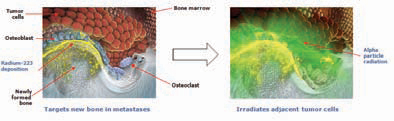
Alpharadin (radium-223 Chloride)
Alpharadin is an intravenous radioactive treatment that hones in on prostate cancer cells that have spread into the bone and irradiates very locally to a small number of cells, as few as 2 to 6.
It has anti-tumor activity without damaging surrounding healthy cells.
Alpharadin uses radiation particles to kill individual cancer cells that can be targeted by chemicals on their surface.
Delivery
In past practice, urologists were handling initial hormonal therapy treatments. But now, these new agents are fraught with more potential side effects, demand informed decision-making and often have delivery methods that need complicated monitoring.
For my busy surgical practice, I have decided that it is more appropriate for medical oncologists to handle patients with advanced prostate cancer who are receiving chemotherapy or other new agents.
Optimism
The proper sequence for administering these agents is not yet clear. Most likely, it will need to be based upon individualized tumor analysis, which is just in beginning stages.
The potential for combining therapies for more effective results certainly exists, but further research is needed to determine how best to do this sequencing and combining.
Explanation:
Hormonal Therapy, Chemotherapy and New Treatments
Primary hormonal therapy involves blocking testosterone production from the testicles.
Secondary hormonal therapy involves blocking testosterone and other androgen production by the adrenal glands and other tissues in the body.
Chemotherapy involves drugs that directly kill cancer cells.
Immunotherapy involves enhancing the host’s immunologic defenses to kill tumor cells containing foreign-appearing tumor antigens.
The new drugs are forms of hormonal therapy that prevent androgens from getting into the nucleus of cancer cells and doing their signaling to cause the tumor cells to grow.
Unfortunately, because of FDA regulatory issues, they have only been tested in men who have failed chemotherapy, so they are only approved for use in men who have failed chemotherapy. However, it would be nice to be able to use them before chemotherapy, but currently we can’t.
Alpharadin uses radiation particles to kill individual cancer cells that can be targeted by chemicals on their surface.






