Dr. Catalona’s Summary and Review of the American Cancer Society’s Estimates of New Cancer Cases in the U.S.
Every year, the American Cancer Society publishes an article on their estimates of the numbers of new cancer cases and deaths in the U.S. This year, they reported the latest results that are the incidence rates (newly diagnosed cases) through 2017, and the mortality rates (cancer deaths per year) through 2018. In 2021, they project 1,898,160 new cancer cases and 608,570 cancer deaths. Before 1991, cancer deaths had been increasing, as fewer people died of heart attacks and strokes and more lived long enough to fall victim to cancer. However, since 1991, there has been a 31% decrease in cancer deaths believed to be due to less smoking and better early detection and treatment of cancer. Prostate cancer deaths have decreased more than any tumor, while death rates also have slowed for breast and colorectal cancers. In contrast, death rates have accelerated for lung cancer.
The COVID-19 pandemic has hampered the diagnosis and treatment of cancer due to closures of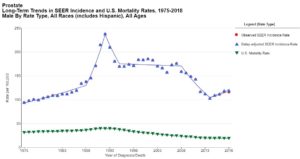 health facilities resulting in delays in diagnosis and treatment. This may lead to a near-term decrease in cancer incidence rates that will be followed by an increase in advanced-stage cases and ultimately increased cancer death rates.
health facilities resulting in delays in diagnosis and treatment. This may lead to a near-term decrease in cancer incidence rates that will be followed by an increase in advanced-stage cases and ultimately increased cancer death rates.
In 2021, prostate, lung, and colorectal cancers comprise 46% of all new cancer cases in men, with prostate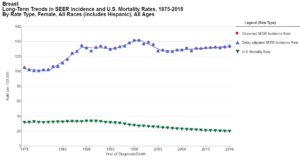 cancer alone accounting for 26% of cases. One man in 8 (12.1%) will be diagnosed with prostate cancer during his lifetime. Breast, lung, and colorectal cancer account for 50% of new cancer cases in women, with breast cancer alone accounting for 30%, and, similarly, 1 woman in 8 (12.9%) will be diagnosed with breast cancer.
cancer alone accounting for 26% of cases. One man in 8 (12.1%) will be diagnosed with prostate cancer during his lifetime. Breast, lung, and colorectal cancer account for 50% of new cancer cases in women, with breast cancer alone accounting for 30%, and, similarly, 1 woman in 8 (12.9%) will be diagnosed with breast cancer.
The incidence rates of prostate cancer decreased dramatically between 2007 to 2014, which is attributed to decreased PSA testing in the wake of US Preventive Services Task Force recommendations against routine screening for prostate cancer because of concerns about over diagnosis and overtreatment. This decision was largely based on flawed clinical trial data that have been criticized for widespread screening among control subjects and insufficient follow-up time. Unfortunately, but not surprisingly, beginning in 2010, the rate of distant-stage prostate cancer diagnoses increased. In 2017, the US Preventive Services Task Force upgraded their recommendation for men aged 55 to 69 years to “informed decision making” about whether or not to screen, and there is evidence that the long-term benefit of screening is underappreciated, particularly given recent advances in mitigating over detection and overtreatment via active surveillance for patients with low-risk disease. Breast cancer incidence rates have continued to increase by about 0.5% per year, which has been attributed in part to reduced fertility rates and obesity.
For all cancer stages combined, survival is highest for prostate cancer (98%) and among the highest for breast cancer (90%). Survival rates are lower for Black patients than for Whites for both prostate and breast cancer. The progress against cancer reflects large decreases in mortality for female breast cancer by 41% (since 1989); for prostate cancer by 52% (since 1993). However, in recent years, mortality declines have slowed for breast cancer and have actually stopped for prostate cancer. For instance, during the late 1990s through 2010, the prostate cancer death rate declined by 4% per year on average because of advances in treatment and earlier stage diagnosis through PSA testing. However, with PSA testing decreasing by about 10 percentage points from 2008 to 2013, coinciding with the uptick in distant-stage disease, the mortality trend has remained relatively flat from 2013 to 2018. It is crucial not to allow the progress in cancer to diminish. It is important to encourage early detection through intelligent, tailored screening and appropriate safe and effective patient management.
Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer Statistics, 2021. CA Cancer J Clin. 2021 Jan;71(1):7-33. doi: 10.3322/caac.21654. Epub 2021 Jan 12. Erratum in: CA Cancer J Clin. 2021 Jul;71(4):359. PMID: 33433946.




















